



Dr. Jin Li: Interpreting the New Findings of CheckMate-8HW — Entering the Era of Dual Immunotherapy for Advanced MSI-H/dMMR Colorectal Cancer
2025-4-15In recent years, immunotherapy has emerged as a major innovative force transforming colorectal cancer (CRC) treatment. This is especially true for patients with metastatic microsatellite instability-high/deficient mismatch repair (MSI-H/dMMR) CRC, a population particularly responsive to immunotherapy. However, unmet needs remain under current PD-1 monotherapy standards. At the 2025 ASCO Gastrointestinal Cancers Symposium (ASCO GI), the CheckMate-8HW study— the first global confirmatory phase III trial exploring nivolumab plus ipilimumab in MSI-H/dMMR metastatic CRC—released groundbreaking data. For the first time, dual immune checkpoint inhibition showed significantly superior benefits compared to monotherapy, establishing a new treatment paradigm and offering renewed hope for patients. In this article, Professor Jin Li of Shanghai GoBroad Cancer Hospital, the principal investigator for China in the CheckMate-8HW study, shares his insights on recent advances in MSI-H/dMMR CRC treatment, the key findings of CheckMate-8HW, and the future of CRC immunotherapy.
1. In recent years, CRC treatment has rapidly evolved, particularly for MSI-H/dMMR patients. Could you summarize recent advances for this patient group?
MSI-H/dMMR CRC patients account for approximately 5% of all CRC cases and represent a distinct subgroup with treatment strategies that differ from those with proficient mismatch repair (pMMR). Notably, they are more responsive to immunotherapy.
In the metastatic setting, the CheckMate-142 study was an initial attempt to evaluate whether dual immune checkpoint inhibition could deliver favorable outcomes and long-term survival. Results showed that first-line treatment with nivolumab plus ipilimumab (O + Y) achieved an objective response rate (ORR) of 71% with low toxicity, outperforming chemotherapy. Building on this, the confirmatory phase III CheckMate-8HW trial was initiated. The findings demonstrated that first-line O + Y therapy for MSI-H/dMMR mCRC patients significantly reduced the risk of disease progression or death compared to chemotherapy, with promising efficacy and a tolerable safety profile, providing an effective treatment option for these patients.
2. The CheckMate-8HW study is particularly important for advanced CRC patients. As the Chinese lead investigator, could you explain its data and the mechanistic advantages of dual immunotherapy?
It was an honor to serve as the Chinese lead investigator for the CheckMate-8HW trial. This randomized, multicenter, open-label phase III trial evaluated the efficacy and safety of O + Y versus nivolumab monotherapy (O) or chemotherapy in MSI-H/dMMR mCRC patients. The co-primary endpoints were progression-free survival (PFS) as assessed by blinded independent central review (BICR) for O + Y versus chemotherapy in the first-line setting, and for O + Y versus O across all lines of therapy (Figure 1).
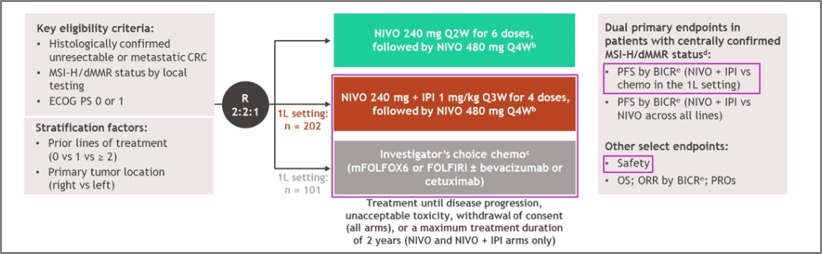
Figure1. Study Design of CheckMate-8HW
At ASCO GI 2024, data showed that the median PFS for the dual immunotherapy group was not reached (NR), while the chemotherapy group had a median PFS of only 5.9 months. O + Y reduced the risk of disease progression or death by 79% (HR 0.21; 95% CI: 0.13–0.35; P < 0.0001), with 2-year PFS rates of 72% vs 14% respectively (Figure 2). This is the first phase III study to confirm the clinical superiority of dual immune checkpoint inhibition over standard chemotherapy for first-line treatment of MSI-H/dMMR mCRC, highlighting its potential for broad clinical application.
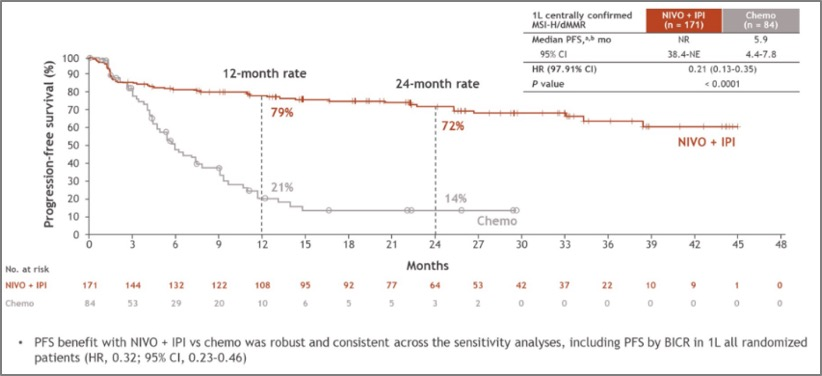
Figure2. PFS for the O + Y dual immunotherapy group and chemotherapy group
Further results presented at ASCO GI 2025 compared O + Y with O monotherapy, showing a minimum follow-up of 16.7 months. The median PFS was NR for O + Y vs 39.3 months for O, with a 38% reduction in risk of progression or death (HR 0.62; 95% CI: 0.48–0.81; P = 0.0003) (Figure 3). ORR was also significantly improved in the O + Y group (71% vs 58%, P = 0.0011), delivering striking clinical data.
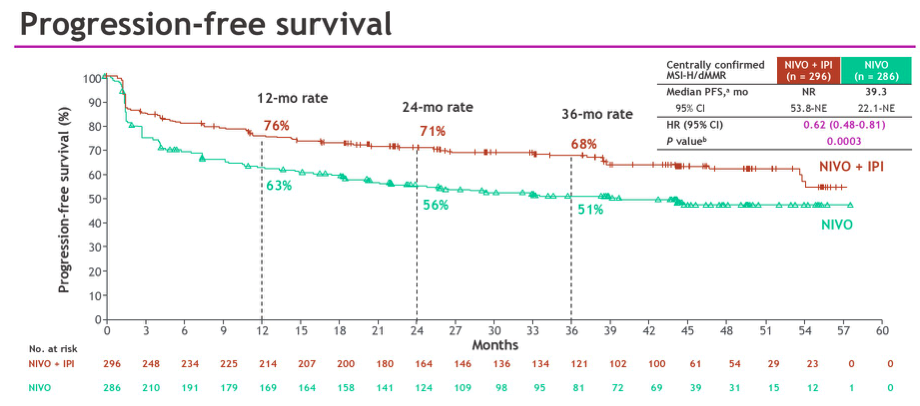
Figure3. Comparison of PFS results between the O + Y group and the O group
Based on these findings, China’s National Medical Products Administration (NMPA) approved O + Y as a first-line treatment for advanced MSI-H/dMMR CRC in October 2024—the first global regulatory approval for this indication. This underscores the openness and patient-centered approach of China's regulatory system.
The impressive results of CheckMate-8HW are closely tied to the synergistic mechanism of dual immunotherapy. Mechanistically, CTLA-4 acts in the early phase of immune activation by being expressed on dendritic cells (DCs) and regulatory T cells (Tregs), suppressing excessive T cell activation and proliferation. Blocking CTLA-4 enhances CD8+ T cell proliferation and activation. Meanwhile, PD-1 functions during the later phase, inhibiting T cell response via PD-L1 on tumor cells. Blocking PD-1 restores T cell recognition and cytotoxicity. Thus, combining CTLA-4 and PD-1 inhibitors yields complementary and durable antitumor effects.
3. Earlier studies have shown the overall tolerability of dual immunotherapy. Based on the latest CheckMate-8HW safety data, what precautions should clinicians take when applying this approach?
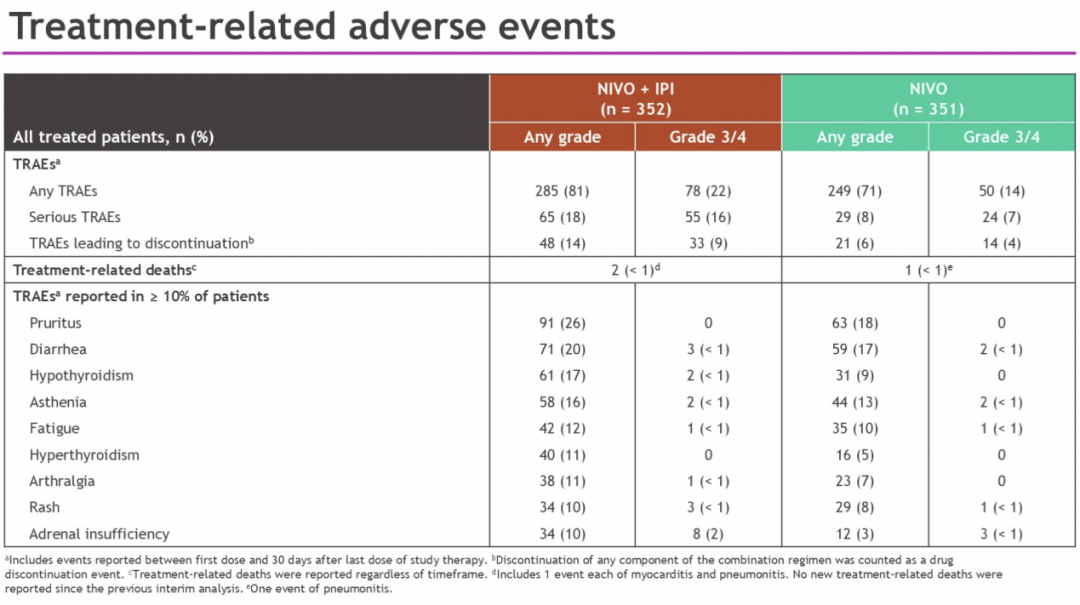
The CheckMate-8HW study demonstrated that O + Y had a favorable safety profile, with no new safety signals. ASCO GI 2024 data showed that grade 3/4 treatment-related adverse events (TRAEs) occurred less frequently with dual immunotherapy than with chemotherapy (23% vs 48%). ASCO GI 2025 further showed comparable safety between O + Y and O monotherapy, with grade 3/4 TRAEs of 22% vs 14%. These were consistent with the 2024 safety data comparing dual immunotherapy to chemotherapy (Table 1).
Table1. Treatment-related Aes
In real-world clinical practice, managing adverse events scientifically is essential. Prevention starts with baseline assessments to identify high-risk patients for immune-related adverse events (irAEs). Patient education is also critical—patients should be informed about symptoms and encouraged to report them early. During treatment, close monitoring and dynamic follow-up are needed for early detection and differential diagnosis of irAEs. Once irAEs occur, timely grading and appropriate interventions—such as corticosteroids or dose adjustments—should be implemented to mitigate severity.
4. Currently, O + Y is primarily used for advanced CRC. What other directions do you foresee for this approach in CRC treatment?
Neoadjuvant therapy is an expanding frontier in CRC. For rectal cancer, where organ preservation is a goal, clinicians are exploring whether effective tumor shrinkage via systemic therapy—possibly combined with radiotherapy—can obviate the need for surgery or reduce surgical extent. The NICHE-2 study has shown encouraging results for neoadjuvant O + Y in dMMR locally advanced CRC, with 3-year follow-up data revealing a major pathologic response (MPR) rate of 95%, pathologic complete response (pCR) rate of 68%, and disease-free survival (DFS) rate of 100%. This suggests that many dMMR patients may not require surgery in the future, achieving both organ and functional preservation through immunotherapy.
Meanwhile, we must also focus on the pMMR population, which comprises the majority of CRC patients. These patients have a response rate of ~50% to chemotherapy plus targeted agents, with a median PFS of 8–10 months. Whether adding dual immunotherapy to chemotherapy could further improve outcomes in pMMR CRC—and under what conditions—remains an open question. More high-quality studies are needed to address these challenges and deliver optimized treatment strategies.
Conclusion
The remarkable efficacy and broad applicability of the O + Y dual immunotherapy regimen represent a new benchmark in the treatment of metastatic CRC, particularly MSI-H/dMMR patients. This approach is reshaping the therapeutic landscape and is expected to set a new standard for first-line therapy. Moving forward, continued exploration of dual immunotherapy across different CRC treatment stages and tumor types, along with accumulation of real-world evidence, will bring even greater benefits to cancer patients.











