


Dr. Zhang Yajing: A New Paradigm in Cytokine Release Syndrome (CRS) Management
2025-7-91. In recent years, CAR-T cell therapy has represented a paradigm shift in cancer immunotherapy. However, we know it comes with certain risks, most notably cytokine release syndrome (CRS), a CAR-T cell-associated toxicity. Could you first share with us the underlying mechanisms of CRS? In your clinical experience, what is the incidence and typical clinical presentation of CRS?
Prof. Zhang Yajing: The pathogenesis of CRS involves a cascade of immune activation events primarily driven by the interaction between CAR-T cells and tumor antigens. This begins when infused CAR-T cells specifically recognize tumor cell surface antigens (such as CD19), activating the T cells through both primary and co-stimulatory signals. The activated CAR-T cells then release perforin and granzyme to lyse tumor cells. This process induces the secretion of pro-inflammatory cytokines such as IL-2, IFN-γ, and TNF-α, which further activate bystander immune cells like monocytes and macrophages, triggering a cytokine cascade. This systemic inflammatory response may result in endothelial permeability and multi-organ dysfunction.
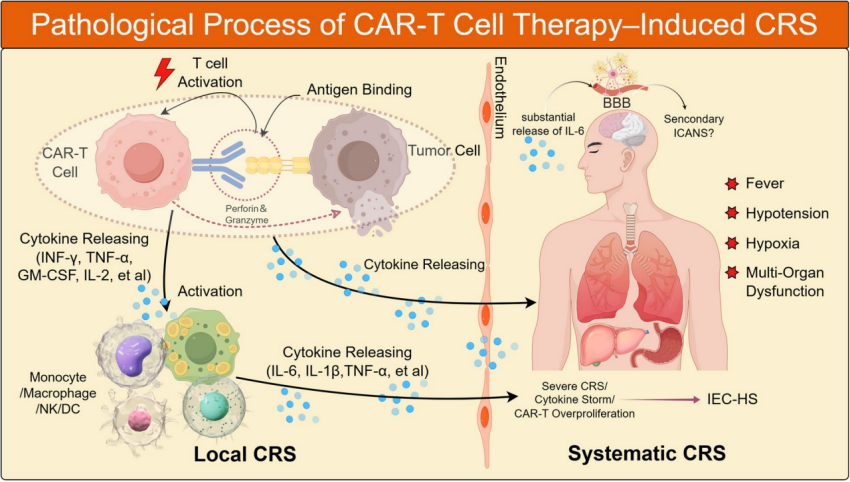
The pathological process of CRS induced by CAR-T therapy
Comprehensive clinical management throughout the CAR-T treatment process is essential for mitigating adverse effects and ensuring treatment safety. Thanks to improved manufacturing techniques and optimized clinical protocols, most patients now experience only mild CRS—typically presenting as fever, fatigue, or myalgia—while the incidence of severe events such as hypotension and hypoxemia has significantly declined. Even in high-risk patients, the proportion requiring intensive care measures such as mechanical ventilation or plasmapheresis has decreased due to improved clinical experience.
As a result, with early recognition, accurate grading, and timely intervention, CRS has become a manageable and controllable adverse effect in the full-cycle management of CAR-T therapy.
2. For different patient populations—such as children, frail elderly individuals, or various disease types—what are the key considerations in devising prevention and treatment strategies? Which medications or regimens does your team currently prefer in clinical practice?
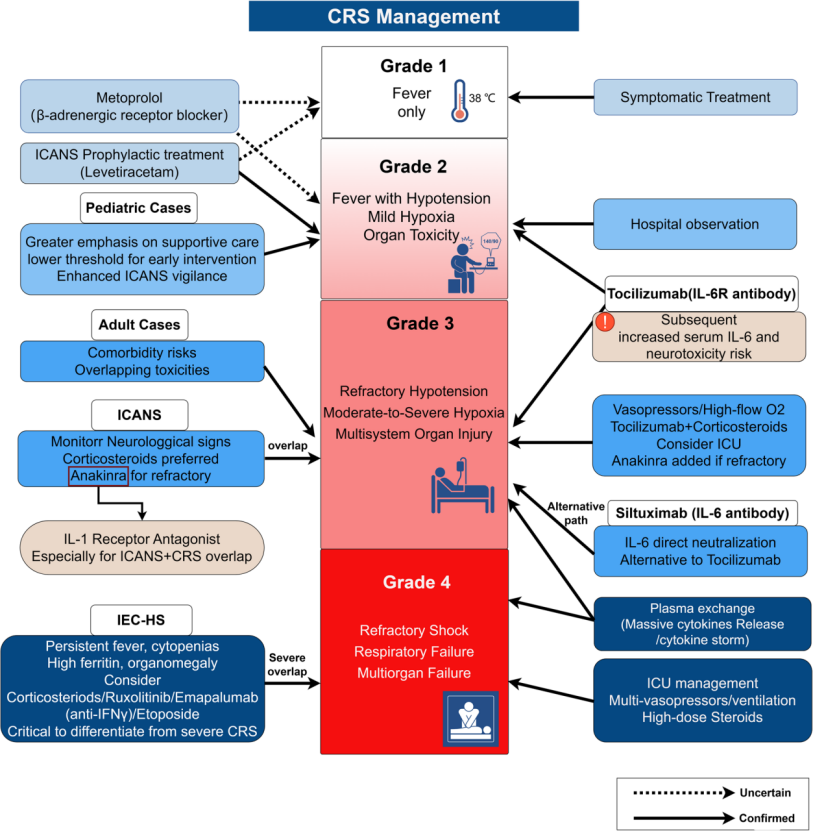
Prof. Zhang Yajing: CRS prevention and treatment should follow the principle of personalized precision medicine rather than a “one-size-fits-all” approach. Current guidelines advocate for graded management tailored to individual patient characteristics.
Stratification of treatment populations is critical. Children and adolescents typically have better organ reserve and can tolerate higher cytokine burdens. In young leukemia patients who are prone to early, intense CRS reactions, optimizing CAR-T efficacy must be balanced with proactive monitoring of organ function. In contrast, frail elderly patients may experience severe consequences from even mild CRS, including multi-organ failure. For these patients, early intervention is essential—such as preemptive use of antibody therapies or low-dose corticosteroids to control CRS severity.
Disease-specific differences also influence CRS management strategies. For example, in acute B-cell leukemia, widespread distribution of tumor cells in bone marrow and peripheral blood means that CAR-T cells encounter targets immediately after infusion, often triggering a rapid and intense CRS. Therefore, early management is critical. Conversely, in lymphoma and multiple myeloma, immunological barriers delay CAR-T expansion until days 5–10 post-infusion, requiring time-adjusted CRS intervention strategies.
Guidelines emphasize the importance of anticipating CRS onset and intervening effectively. First and foremost, supportive care must be optimized. Since infection combined with CRS carries high mortality, it's essential to control any active infection before CAR-T infusion.
Beyond IL-6 receptor antagonists and steroids, additional therapeutic options are now available. Our foundational research has shown that β-blockers like metoprolol can reduce IL-6 production and alleviate CRS severity without impairing CAR-T function. Moreover, IL-1 receptor antagonists and antibodies targeting TNF-α or IFN-γ have shown promise in controlling CRS while maintaining CAR-T expansion.
In high tumor burden or leukemia patients with grade ≥3 CRS and massive cytokine release, plasmapheresis may be used to rapidly clear inflammatory mediators and restore homeostasis. For cases of excessive CAR-T proliferation and cytokine release, tyrosine kinase inhibitors such as dasatinib can serve as a pharmacologic “off switch” to temporarily suppress CAR-T activity, helping patients safely navigate the critical period and improve outcomes.
3. You mentioned the importance of multidisciplinary collaboration in CRS management. How does your institution coordinate among departments to manage CRS? Could you share any standardized procedures or SOPs?
Prof. Zhang Yajing: Multidisciplinary collaboration is central to safely implementing CAR-T therapy. Both international guidelines and domestic clinical practice emphasize full-cycle management via a multidisciplinary team (MDT). In addition to hematology, departments involved include critical care, infectious disease, pulmonology, pharmacy, neurology, and nursing. Their collaboration is key to precise adverse event prevention and management.
Timing of interdisciplinary engagement is equally vital. During patient selection, teams assess risk based on tumor biology, aggressiveness, and burden. Early involvement from the ICU team helps with risk stratification. Throughout treatment, infection prevention is crucial, especially as bridging and conditioning regimens cause bone marrow suppression. After CAR-T infusion, infection risks spike, necessitating protective isolation and close monitoring of infection markers such as CRP, procalcitonin, and NGS (next-generation sequencing). Infectious disease support is essential in these measures.
Multidisciplinary collaboration forms a closed-loop management system for risk prediction, rapid identification, and timely intervention. For example, timely plasmapheresis or hemofiltration can improve outcomes during cytokine storms. With the support of an MDT, the safety and effectiveness of CAR-T treatment can be maximized for patient benefit.
4. With ongoing advances in cellular therapy, what future directions do you foresee in CRS prevention and management? Which areas or novel therapeutics are likely to see breakthroughs?
Prof. Zhang Yajing: While clinical experience in CAR-T therapy is growing, there are key challenges yet to be resolved. Scientifically, we need deeper exploration into CRS molecular mechanisms—beyond the well-known IL-6, IFN-γ, and TNF-α—to include IL-18, IL-15, IL-1, and various chemokines and their interactions with specific cell populations.
Emerging research is also focused on identifying predictive biomarkers for CRS. This could lead to targeted therapeutics and proactive, full-cycle CRS prevention strategies.
Artificial intelligence (AI) is offering new possibilities. By integrating proteomics, single-cell sequencing, and multi-omics analysis with AI-based models, we can move from reactive management to proactive prediction—allowing early identification of at-risk patients and timely clinical decision-making.
On the technical front, innovation in CAR-T cell structure and production is ongoing. Suicide genes or molecular switches are being developed to externally control CAR-T cell activity. “Armored” CAR-T cells can retain tumor-killing potency while modulating cytokine release. Emerging technologies like E-CARs, CAR-NK, and universal CAR-γδ T cells represent a shift toward “smarter, safer” cell therapies. These innovations mark major milestones in advancing the safety and intelligence of cell therapy.
Summary
CRS is a common treatment-related reaction in CAR-T therapy. Although it poses significant challenges, deepening our understanding of pathophysiology, implementing personalized risk stratification, establishing standardized MDT protocols, and incorporating cutting-edge technologies have collectively improved the safety and efficacy of CAR-T therapy.
Looking ahead, the development of predictive biomarkers, risk modeling, and next-generation cell therapy platforms will continue to refine clinical strategies—allowing more patients to benefit from this revolutionary treatment and advancing the mission of extending life through medical innovation.












